Thursday April 30, 2009
Q: What is the half life of Argatroban?
Answer: About 50 minutes
As Argatroban is metabolized in the liver, assuming patient has a normal liver function, its half life is about 50 minutes. It is monitored by PTT in same way as heparin drip.
In contrast, lepirudin, another direct thrombin inhibitor is primarily cleared by kidneys and should be either avoided or adjusted with renal insufficiency.
Thursday, April 30, 2009
Wednesday, April 29, 2009
Monday, April 27, 2009
Monday April 27, 2009
Lactic acid level is still very relevant
Serum lactate is a potentially useful biomarker to risk-stratify patients with severe sepsis. Objective of this study to test whether the association between initial serum lactate level and mortality in patients presenting to the emergency department (ED) with severe sepsis is independent of organ dysfunction and shock. It was a single-center cohort study of 830 patients at an ED of an academic tertiary care center from 2005 to 2007. who were admitted with severe sepsis.
The primary outcome: 28-day mortality
Risk factor variable: Initial venous lactate (mmol/L), categorized as
Potential covariates: age, sex, race, acute and chronic organ dysfunction, severity of illness, and initiation of early goal-directed therapy.
Results:
Conclusions: Initial serum lactate was associated with mortality independent of clinically apparent organ dysfunction and shock in patients admitted to the ED with severe sepsis. Both intermediate and high serum lactate levels were independently associated with mortality.
Reference: click to get abstract
Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock - Critical Care Medicine. 37(5):1670-1677, May 2009
Lactic acid level is still very relevant
Serum lactate is a potentially useful biomarker to risk-stratify patients with severe sepsis. Objective of this study to test whether the association between initial serum lactate level and mortality in patients presenting to the emergency department (ED) with severe sepsis is independent of organ dysfunction and shock. It was a single-center cohort study of 830 patients at an ED of an academic tertiary care center from 2005 to 2007. who were admitted with severe sepsis.
The primary outcome: 28-day mortality
Risk factor variable: Initial venous lactate (mmol/L), categorized as
- low (less than 2),
- intermediate (2-3.9), or
- high (more than/=4)
Potential covariates: age, sex, race, acute and chronic organ dysfunction, severity of illness, and initiation of early goal-directed therapy.
Results:
- Mortality at 28 days was 22.9% and
- Median serum lactate was 2.9 mmol/L.
- Intermediate and high serum lactate levels were associated with mortality in the nonshock subgroup.
- In the shock subgroup, intermediate and high serum lactate levels were also associated with mortality.
Conclusions: Initial serum lactate was associated with mortality independent of clinically apparent organ dysfunction and shock in patients admitted to the ED with severe sepsis. Both intermediate and high serum lactate levels were independently associated with mortality.
Reference: click to get abstract
Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock - Critical Care Medicine. 37(5):1670-1677, May 2009
Sunday, April 26, 2009
Sunday April 26, 2009
Q; Thrombotic thrombocytopenic purpura (TTP) is an occasional but serious side effect of PLAVIX® (clopidogrel bisulfate). Why its important to quickly recognize this side effect?
Answer: Its very important to recognise Clopidogrel associated TTP. It usually occurs within 2 weeks of start of treatment. Beside discontinuation of drug, total plasma exchange (TPE) should be initiated as soon as possible.
Persons who received plasma exchange within 3 days of TTP onset were more likely to survive than those in whom plasma exchange was initiated after 3 days (survival rate, 100% versus 27.3%)
Reference: click to get article
Clopidogrel-Associated TTP - Stroke. 2004;35:533.
Q; Thrombotic thrombocytopenic purpura (TTP) is an occasional but serious side effect of PLAVIX® (clopidogrel bisulfate). Why its important to quickly recognize this side effect?
Answer: Its very important to recognise Clopidogrel associated TTP. It usually occurs within 2 weeks of start of treatment. Beside discontinuation of drug, total plasma exchange (TPE) should be initiated as soon as possible.
Persons who received plasma exchange within 3 days of TTP onset were more likely to survive than those in whom plasma exchange was initiated after 3 days (survival rate, 100% versus 27.3%)
Reference: click to get article
Clopidogrel-Associated TTP - Stroke. 2004;35:533.
Saturday, April 25, 2009
Saturday April 25, 2009
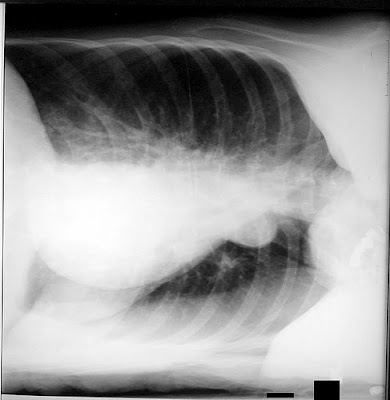
Q; 58 Year old male with history of ETOH abuse, drug abuse and malnutrition is admitted to ICU with drug overdose. Patient required intubation for protection of airway. Post-intubation CXR is below. Your concern/diagnosis?
Q; 58 Year old male with history of ETOH abuse, drug abuse and malnutrition is admitted to ICU with drug overdose. Patient required intubation for protection of airway. Post-intubation CXR is below. Your concern/diagnosis?

Answer: Tooth in Right main bronchus
Malnourished patients with poor dentition are prone to loose teeth during intubation. Tootth should be removed immediately with bronchoscopy to avoid any complication like pneumonia, perforation, atelactasis etc. It may be surprising but this is one of the very few dental emergency in ICU as an intact tooth can be reimplanted and saved, if performed within an hour. Tooth should be saved in normal saline and oral surgeon should be called immediately.
Friday, April 24, 2009
Friday April 24, 2009 (pediatric pearl day)
Extracorporeal life support in children with acute respiratory failure
Among children with acute respiratory failure higher survival to hospital discharge were seen in :
- younger patient age;
- fewer days of mechanical ventilation before ECLS;
- lower PIP;
- higher Pao2/Fio2 ratio;
- higher pH;
- recent era (post-1996);
- no use of iNO; and
- no immunocompromising diagnosis
(all p values less than .05)
These variables were obtained on the analysis of the ELSO registry (contains data from more than145 centers worldwide that contributed information on ECLS for severe respiratory or cardiac failure) contained 2,879 pediatric patients between 1 month and 19 yrs of age who were treated with ECLS for respiratory failure.
Reference:
Extracorporeal life support for severe respiratory failure in children with immune compromised conditions - Pediatric Critical Care Medicine. 9(4):380-385, July 2008.Pediatr Crit Care 2008; 9(4); 380-385
Thursday, April 23, 2009
Thursday April 23, 2009
Q: Treatment of steroid psychosis is?
A) Mellaril (Thioridazine)
B) Thorazine (Chlorpromazine)
C) Haloperidol
D) All of the above
Answer is E
Steroid psychosis is very common in ICUs and unfortunately often go undiagnosed. It occurs in about 5% of patients receiving steroids for other medical reasons. Physician usually has a window of 1-3 days to abort the full-blown picture of steroid psychosis. Discontinuation of steroids, supportive treatment and psychotropic medications are needed.
Treatment include Mellaril 50 to 200mg q.d.; Thorazine 50 to 200mg p.o., q.d. or Haloperidol 2 to 10mg p.o., q.d.
Symptoms of steroid psychosis sits on a wide range of spectrum including profound distractibility, pressured speech, anxiety, emotional lability, severe insomnia, sensory flooding, depression, perplexity, hallucinations, agitation, intermittent memory impairment, mutism, delusions, disturbances of body image, apathy and hypomania.
Reference:
1. Corticosteroid-Induced Psychotic and Mood Disorders - Psychosomatics 42:461-466, December 2001
2. Psychiatric Adverse Drug Reactions: Steroid Psychosis - lecture of Richard C.W. Hall, M.D.
Q: Treatment of steroid psychosis is?
A) Mellaril (Thioridazine)
B) Thorazine (Chlorpromazine)
C) Haloperidol
D) All of the above
Answer is E
Steroid psychosis is very common in ICUs and unfortunately often go undiagnosed. It occurs in about 5% of patients receiving steroids for other medical reasons. Physician usually has a window of 1-3 days to abort the full-blown picture of steroid psychosis. Discontinuation of steroids, supportive treatment and psychotropic medications are needed.
Treatment include Mellaril 50 to 200mg q.d.; Thorazine 50 to 200mg p.o., q.d. or Haloperidol 2 to 10mg p.o., q.d.
Symptoms of steroid psychosis sits on a wide range of spectrum including profound distractibility, pressured speech, anxiety, emotional lability, severe insomnia, sensory flooding, depression, perplexity, hallucinations, agitation, intermittent memory impairment, mutism, delusions, disturbances of body image, apathy and hypomania.
Reference:
1. Corticosteroid-Induced Psychotic and Mood Disorders - Psychosomatics 42:461-466, December 2001
2. Psychiatric Adverse Drug Reactions: Steroid Psychosis - lecture of Richard C.W. Hall, M.D.
Wednesday, April 22, 2009
Tuesday, April 21, 2009
Tuesday April 21, 2009
Site of Action of Antimicrobials - in nutshell
Cell Wall
Beta Lactams: Penicillins, Cephalosporins, Monobactams, Carbapenems
Glycopeptides: Vancomycin
Lipopeptide (Cell Membrane): Daptomycin
Cytoplasm
Initiation Complex: Linezolid
30S Ribosome: Aminoglycosides, Tetracyclines
50S Ribosome: Macrolides/Ketolides, Chloramphenicol, Clindamycin, Quinupristin-dalfopristin
DNA Inhibitor
Metronidazole, Fluoroquinolones, TMP-SMZ, Rifampin
Site of Action of Antimicrobials - in nutshell
Cell Wall
Beta Lactams: Penicillins, Cephalosporins, Monobactams, Carbapenems
Glycopeptides: Vancomycin
Lipopeptide (Cell Membrane): Daptomycin
Cytoplasm
Initiation Complex: Linezolid
30S Ribosome: Aminoglycosides, Tetracyclines
50S Ribosome: Macrolides/Ketolides, Chloramphenicol, Clindamycin, Quinupristin-dalfopristin
DNA Inhibitor
Metronidazole, Fluoroquinolones, TMP-SMZ, Rifampin
Monday, April 20, 2009
Monday April 20, 2009
Q: Propofol should be given with caution in which common allergy?
A: Egg allergy
Originally propofol was launched 32 years ago but was withdrawn from the market due to reports of anaphylactic reactions. It was re-launched in 1986 by AstraZeneca with the brand name Diprivan with preparation containing 10% soybean oil and 1.2% purified egg lecithin, a phosphatidylcholine found in egg yolk.
A history of egg allergy does not necessarily contraindicate the use of propofol. Most egg allergies are related to a reaction to the egg white (albumin) and not to the egg yolk (lecithin). This could explain why 'propofol' is only very rarely a problem. However, a patient who has an egg allergy should be carefully questioned.
Q: Propofol should be given with caution in which common allergy?
A: Egg allergy
Originally propofol was launched 32 years ago but was withdrawn from the market due to reports of anaphylactic reactions. It was re-launched in 1986 by AstraZeneca with the brand name Diprivan with preparation containing 10% soybean oil and 1.2% purified egg lecithin, a phosphatidylcholine found in egg yolk.
A history of egg allergy does not necessarily contraindicate the use of propofol. Most egg allergies are related to a reaction to the egg white (albumin) and not to the egg yolk (lecithin). This could explain why 'propofol' is only very rarely a problem. However, a patient who has an egg allergy should be carefully questioned.
Sunday, April 19, 2009
Sunday April 19, 2009
Is small doses of Succinylcholine is as good as full dose for tracheal intubation?
Background: Succinylcholine 1.0 mg/kg usually produces excellent tracheal intubation conditions in 60 s. Recovery of respiratory muscle function after this dose, however, is not fast enough to forestall oxyhemoglobin desaturation when ventilation cannot be assisted. In this study, we investigated whether smaller doses of succinylcholine can produce satisfactory intubation conditions fast enough to allow rapid sequence induction with a shorter recovery time.
Method: Anesthesia was induced with fentanyl/propofol and maintained by propofol infusion and N2O in O2. After the induction, 115 patients were randomly allocated to five groups according to the dose of succinylcholine
0.3 mg/kg, 0.4 mg/kg, 0.5 mg/kg, 0.6 mg/kg, or 1.0 mg/kg
Evoked adductor pollicis responses to continuous 1-Hz supramaximal ulnar nerve stimulation were recorded using acceleromyography. Tracheal intubation conditions were graded 60 s after succinylcholine administration. Onset time, maximal twitch depression, time to initial twitch detection after paralysis, and to 10%, 25%, 50%, and 90% twitch height recovery were recorded. Time to initial diaphragmatic movement as well as time to resumption of regular spontaneous respiratory movements were calculated.
Results:
IMPLICATIONS: In normal healthy patients, succinylcholine 0.6 mg/kg produces clinical intubation conditions identical to the traditional 1.0-mg/kg dose but is associated with a shorter recovery time.
Reference: Click to get abstract
The Neuromuscular Effects and Tracheal Intubation Conditions After Small Doses of Succinylcholine Anesth Analg 2004;98:1680-1685
Is small doses of Succinylcholine is as good as full dose for tracheal intubation?
Background: Succinylcholine 1.0 mg/kg usually produces excellent tracheal intubation conditions in 60 s. Recovery of respiratory muscle function after this dose, however, is not fast enough to forestall oxyhemoglobin desaturation when ventilation cannot be assisted. In this study, we investigated whether smaller doses of succinylcholine can produce satisfactory intubation conditions fast enough to allow rapid sequence induction with a shorter recovery time.
Method: Anesthesia was induced with fentanyl/propofol and maintained by propofol infusion and N2O in O2. After the induction, 115 patients were randomly allocated to five groups according to the dose of succinylcholine
0.3 mg/kg, 0.4 mg/kg, 0.5 mg/kg, 0.6 mg/kg, or 1.0 mg/kg
Evoked adductor pollicis responses to continuous 1-Hz supramaximal ulnar nerve stimulation were recorded using acceleromyography. Tracheal intubation conditions were graded 60 s after succinylcholine administration. Onset time, maximal twitch depression, time to initial twitch detection after paralysis, and to 10%, 25%, 50%, and 90% twitch height recovery were recorded. Time to initial diaphragmatic movement as well as time to resumption of regular spontaneous respiratory movements were calculated.
Results:
- Onset times ranged between 82 s and 52 s, decreasing with increasing doses of succinylcholine but not differing between 0.6 and 1 mg/kg.
- Maximum twitch depression was similar after 0.5, 0.6, and 1 mg/kg (98.2%–100%).
- Recoveries of twitch height and apnea time were dose-dependent.
Intubation conditions were often unacceptable after 0.3- and 0.4-mg/kg doses. - Acceptable intubation conditions were achieved in all patients receiving a 0.5, 0.6, and 1 mg/kg dose of succinylcholine.
- Intubation conditions in patients receiving 0.6 and 1 mg/kg were identical, whereas times to T1 = 50% and 90% and time to regular spontaneous reservoir bag movements were significantly shorter in the 0.6-mg/kg dose group (5.78, 7.25, and 4.0 min, respectively) versus patients receiving 1 mg/kg (8.55, 10.54, and 6.16 min, respectively).
Conclusion: The use of 0.5 to 0.6 mg/kg of succinylcholine can produce acceptable intubation conditions 60 s after administration. The conditions achieved after 0.6 mg/kg are similar to those after 1.0 mg/kg. These smaller doses are associated with faster twitch recovery and shorter apnea time.
IMPLICATIONS: In normal healthy patients, succinylcholine 0.6 mg/kg produces clinical intubation conditions identical to the traditional 1.0-mg/kg dose but is associated with a shorter recovery time.
Reference: Click to get abstract
The Neuromuscular Effects and Tracheal Intubation Conditions After Small Doses of Succinylcholine Anesth Analg 2004;98:1680-1685
Friday, April 17, 2009
Friday April 17, 2009 (pediatric pearl)
Altered zinc homeostasis in septic shock
Intact zinc homeostasis must be present for normal function of the immune system, oxidative stress responses, neurocognitive function, and growth and development.
Metallothioneins are cysteine-rich, metal-binding proteins involved in the homeostasis of zinc transcription is strongly down-regulated in the setting of zinc deficiency, but is up-regulated with inflammation, metals, and administration of exogenous glucocorticoids
Plasma zinc concentrations are low in critically ill children.
A correlation between zinc levels and expression of some metallothionein isoforms was observed on day 1, whereas there was no correlation between zinc levels and measures of inflammation such as CRP and IL-6 on day 1. However, by day 3, this trend had reversed itself, such that the correlation with MT levels was no longer present, but plasma zinc was associated with CRP and IL-6 levels.
Also, by day 3 there was a correlation between plasma zinc levels and the degree of organ failure.
It is thought that that enhanced metallothionein expression early in acute stress and the associated decline in plasma zinc contribute to the subsequent inflammatory response and the risk of organ failure in critically ill children.
References: Click to get abstract
1. Genome-level expression profiles in pediatric septic shock indicate a role for altered zinc homeostasis in poor outcome - Physiol. Genomics 30: 146-155, 2007. First published March 20, 2007
2. Zinc homeostasis in pediatric critical illness- Pediatric Critical Care Medicine. 10(1):29-34, January 2009
Thursday, April 16, 2009
Thursday April 16, 2009
Scenario: 42 year old female presented with weakness, ataxia, nausea, slurred speech, dehydration, and severe lethargy. Lab showed high anion gap metabolic acidosis. Patient was made NPO and was resuscitated with IVF and empiric antibiotics. Patient stabalized within 24 hours. Review of old record showed similar multiple episodes with no clear diagnosis before each discharge except for one unrelated admission 12 years ago for uneventful gastric bypass surgery.
Patient "bounced back" to ICU after 2 days with similar clinical presentation. Due to clerical error D-Lactic acid was marked instead of L-Lactic acid on lab slip and indeed it is reported high and patient was diagnosed with "D-Lactic acidosis". What is D-Lactic Acidosis?
Answer: There are 2 kinds of Lactic Acidosis
L-lactate: It is the only form produced in human metabolism, and its excess represents increased anaerobic metabolism due to tissue hypoperfusion.
D-lactate: It is a byproduct of bacterial metabolism and may accumulate in patients with short-gut syndrome or in those with a history of gastric bypass or small-bowel resection.
Development of "D-Lactic acidosis" occurs due to carbohydrate malabsorption with ingestion of large amounts of carbohydrate, and colonic bacterial flora of a type that produces d-lactic acid. It get worse due to diminished colonic motility, allowing time for nutrients in the colon to undergo bacterial fermentation.
Reference: click to get abstract
D-lactic acidosis. A review of clinical presentation, biochemical features, and pathophysiologic mechanisms - Medicine (Baltimore) 1998 Mar;77(2):73-82
Scenario: 42 year old female presented with weakness, ataxia, nausea, slurred speech, dehydration, and severe lethargy. Lab showed high anion gap metabolic acidosis. Patient was made NPO and was resuscitated with IVF and empiric antibiotics. Patient stabalized within 24 hours. Review of old record showed similar multiple episodes with no clear diagnosis before each discharge except for one unrelated admission 12 years ago for uneventful gastric bypass surgery.
Patient "bounced back" to ICU after 2 days with similar clinical presentation. Due to clerical error D-Lactic acid was marked instead of L-Lactic acid on lab slip and indeed it is reported high and patient was diagnosed with "D-Lactic acidosis". What is D-Lactic Acidosis?
Answer: There are 2 kinds of Lactic Acidosis
L-lactate: It is the only form produced in human metabolism, and its excess represents increased anaerobic metabolism due to tissue hypoperfusion.
D-lactate: It is a byproduct of bacterial metabolism and may accumulate in patients with short-gut syndrome or in those with a history of gastric bypass or small-bowel resection.
Development of "D-Lactic acidosis" occurs due to carbohydrate malabsorption with ingestion of large amounts of carbohydrate, and colonic bacterial flora of a type that produces d-lactic acid. It get worse due to diminished colonic motility, allowing time for nutrients in the colon to undergo bacterial fermentation.
Reference: click to get abstract
D-lactic acidosis. A review of clinical presentation, biochemical features, and pathophysiologic mechanisms - Medicine (Baltimore) 1998 Mar;77(2):73-82
Wednesday, April 15, 2009
Wednesday April 15, 2009
Diagnostic Criteria for Portopulmonary Hypertension (POPH)
Specific diagnostic criteria for POPH obtained by right heart catheterization have been espoused by the European Respiratory Society Task Force on Pulmonary-Hepatic Vascular Disorders
Related: Power point presentation on POPH (George T. Kondos, MD)
Reference: click to get abstract
Rodriguez-Roisin R, Krowka MJ, Herve P, Fallon MB. Pulmonary-hepatic vascular disorders: a task force report. Eur Respir J. 2004;24:861-880.
Diagnostic Criteria for Portopulmonary Hypertension (POPH)
Specific diagnostic criteria for POPH obtained by right heart catheterization have been espoused by the European Respiratory Society Task Force on Pulmonary-Hepatic Vascular Disorders
- Presence of portal hypertension (clinical diagnosis)A) With or without cirrhosis
- Mean pulmonary artery pressure (mPAP) > 25 mm Hg
- Pulmonary vascular resistance (PVR) > 240 dynes sec/cm-5
- Transpulmonary gradient* > 12 mm Hg
*Transpulmonary gradient = mean pulmonary artery pressure - pulmonary artery occlusion pressure (mPAP - PAOP).
Related: Power point presentation on POPH (George T. Kondos, MD)
Reference: click to get abstract
Rodriguez-Roisin R, Krowka MJ, Herve P, Fallon MB. Pulmonary-hepatic vascular disorders: a task force report. Eur Respir J. 2004;24:861-880.
Tuesday, April 14, 2009
Tuesday April 14, 2009
Prone positioning in hypoxemic respiratory failure:
Meta-analysis of randomized controlled trials
We have seen the ups and down of prone ventilation. Kopterides did the meta-analysis to assess the effect of prone positioning on intensive care unit (ICU) and hospital mortality, days on mechanical ventilation, length of stay, incidence of ventilator-associated pneumonia (VAP) and pneumothorax, and associated complications.
Result:
Conclusion: This meta-analysis revealed that prone positioning does not change the overall mortality, but may have benefit in the selected group of severely ill patients. It decreases the incidence of VAP, but has more pressure sores and endotracheal tube related complications.
Reference: click to get abstract
Kopterides P, Siempos I, Armaganidis A. Prone positioning in hypoxemic respiratory failure: Meta-analysis of randomized controlled trials. J of Critical Care 2009; 24(1): 89-100
Prone positioning in hypoxemic respiratory failure:
Meta-analysis of randomized controlled trials
We have seen the ups and down of prone ventilation. Kopterides did the meta-analysis to assess the effect of prone positioning on intensive care unit (ICU) and hospital mortality, days on mechanical ventilation, length of stay, incidence of ventilator-associated pneumonia (VAP) and pneumothorax, and associated complications.
Result:
- The pooled odds ratio (OR) for the ICU mortality in the intention-to-treat analysis was 0.97 (95% confidence interval [CI], 0.77-1.22), for the comparison between prone and supine ventilated patients
- The pooled OR for the ICU mortality in the more severely ill patients favored prone positioning (OR, 0.34; 95% CI, 0.18-0.66)
- The duration of mechanical ventilation and the incidence of pneumothorax were not different between the 2 groups
- The incidence of VAP was lower but not statistically significant in patients treated with prone positioning (OR, 0.81; 95% CI, 0.61-1.10)
(However)
- Prone positioning was associated with a higher risk of pressure sores (OR, 1.49; 95% CI, 1.17-1.89) and
- Prone positioning was associated with a trend for more complications related to the endotracheal tube (OR, 1.30; 95% CI, 0.94-1.80)
Conclusion: This meta-analysis revealed that prone positioning does not change the overall mortality, but may have benefit in the selected group of severely ill patients. It decreases the incidence of VAP, but has more pressure sores and endotracheal tube related complications.
Reference: click to get abstract
Kopterides P, Siempos I, Armaganidis A. Prone positioning in hypoxemic respiratory failure: Meta-analysis of randomized controlled trials. J of Critical Care 2009; 24(1): 89-100
Monday, April 13, 2009
Monday April 13, 2009
Meld Score: What is it?
It is a model for End-Stage Liver Disease, initially designed and validated for predicting survival in patients with portal hypertension undergoing TIPS (transjugular intrahepatic portosystemic shunt).
Three things used in calculating the predicting models are
1. INR (international normalized ratio)
2. Serum creatinine
3. Serum Bilirubin
It is calculated as
MELD=9.57 x loge (creatinine) + 3.78 loge (total bilirubin) + 11.2 Loge (INR) =6.43
It has played an important role in predicting the mortality in liver disease, and has significantly decreased the liver transplantation time. Patient with Meld score of less than 16 has good survival, and score of more than 24 has poor survival. It also removes favoritism and subjective bias out of transplant preference.
Reference: click to get abstract
Kamath PS, Kim WR. The model for end stage liver disease (MELD). Hepatology 2007; 45(3): 797-805
Meld Score: What is it?
It is a model for End-Stage Liver Disease, initially designed and validated for predicting survival in patients with portal hypertension undergoing TIPS (transjugular intrahepatic portosystemic shunt).
Three things used in calculating the predicting models are
1. INR (international normalized ratio)
2. Serum creatinine
3. Serum Bilirubin
It is calculated as
MELD=9.57 x loge (creatinine) + 3.78 loge (total bilirubin) + 11.2 Loge (INR) =6.43
It has played an important role in predicting the mortality in liver disease, and has significantly decreased the liver transplantation time. Patient with Meld score of less than 16 has good survival, and score of more than 24 has poor survival. It also removes favoritism and subjective bias out of transplant preference.
Reference: click to get abstract
Kamath PS, Kim WR. The model for end stage liver disease (MELD). Hepatology 2007; 45(3): 797-805
Sunday, April 12, 2009
Sunday April 12, 2009
Scenario: 67 yeear old male is now stable after his acute MI and cardiogenic shock. Patient is now 'delined' and 'detubed' and stable to transfer to floor. Whie reviewing morning CXR, you had following picture. Whats your diagnosis ?

Answer: Swan ganz catheter fragment which has broken loose and ended up in the right pulmonary artery.
Interventional Radiologist can remove the lost catheter via procedure call Snare Technique. This is done percutaneously, through a skin incision in the groin under local anesthesia. But Cardio-thoracic surgery should be taken on consult as backup, in case it requires open heart method.
Reference: click to get abstract
Embolization of the Tip of a Central Venous Catheter into the Pulmonary Artery - NEJM - Volume 352:e3 January 27, 2005 Number 4
Scenario: 67 yeear old male is now stable after his acute MI and cardiogenic shock. Patient is now 'delined' and 'detubed' and stable to transfer to floor. Whie reviewing morning CXR, you had following picture. Whats your diagnosis ?
Answer: Swan ganz catheter fragment which has broken loose and ended up in the right pulmonary artery.
Interventional Radiologist can remove the lost catheter via procedure call Snare Technique. This is done percutaneously, through a skin incision in the groin under local anesthesia. But Cardio-thoracic surgery should be taken on consult as backup, in case it requires open heart method.
Reference: click to get abstract
Embolization of the Tip of a Central Venous Catheter into the Pulmonary Artery - NEJM - Volume 352:e3 January 27, 2005 Number 4
Saturday, April 11, 2009
Saturday April 11, 2009
Regarding pleural effusions
Scenario: 67 yeear old male presented to ER with shortness of breath. There is significant opacification of left lateral lobe. Your dignosis is pleural effusion with underlying atelactasis. To acertain reasonable amount of fluid to tap (thoracentesis), what could be your next step?

Regarding pleural effusions
Scenario: 67 yeear old male presented to ER with shortness of breath. There is significant opacification of left lateral lobe. Your dignosis is pleural effusion with underlying atelactasis. To acertain reasonable amount of fluid to tap (thoracentesis), what could be your next step?
Answer: Perform lateral decubitus films
CXRs done in the lateral decubitus position are more sensitive, and can pick up as little as 50 ml of fluid. Upright chest films need at least 300 ml of fluid to pick up pleural effusion consistent with blunting of costophrenic angles. If the fluid layer is more than 1 cm, there is enough of it to do a pleural tap. Lateral decubitus film may also help in revealing loculated pleural effusions, if any - which may require CT-guided thoracocentesis. 500 ml of pleural effusion is enough to show detectable clinical signs.

Friday, April 10, 2009
Friday April 10, 2009 (pediatric pearl)
Risk factors of upper gastrointestinal bleeding in mechanically ventilated children
Overt upper gastrointestinal bleeding* is common of critically ill children requiring mechanical ventilation (52%).
Significant upper gastrointestinal bleeding*1 is uncommon (3.6%) (Similar to that seen in adults studies).
60% of patients with UGI bleeding occurred on the first day and more than 90% occurred within the first 3 days.
*Overt upper gastrointestinal bleeding = evidence of hematemesis, gross blood, or “coffee ground” material in nasogastric aspirates, hematochezia, or melena
*1 Significant UGI bleeding = defined as a spontaneous decrease of more than 20 mm Hg in the systolic blood pressure, an increase of more than 20 beats per minute in the heart rate, a decrease in the hemoglobin level of more than 2 g/dL, the receipt of packed red blood cell transfusion and gastric or duodenal surgery.
Reference: click to get abstract
Incidence and risk factors of upper gastrointestinal bleeding in mechanically ventilated children - Pediatric Critical Care Medicine. 10(1):91-95, January 2009
Thursday, April 9, 2009
Wednesday, April 8, 2009
Wednesday April 8, 2009
Resistance to Heparin Therapy
Q; What is the most common reason of Resistance to Heparin Therapy (failure of monitoring tests to change or higher than expected doses) ?
Answer: The most important cause of apparent resistance to heparin therapy is antithrombin III deficiency. Replacement of antithrombin III in a deficient patient may restore heparin efficacy.
Also, its important to know that following commonly use medicines may cause resistance to heparin therapy.
- intravenous nitroglycerin
- digitalis,
- nicotine (smoking),
- tetracycline
- some antihistamines
Reference:
Bick RL., Disorders of Thrombosis & Hemostasis. Clinical and Laboratory Practice. 1992. ASCP Press. (Figure 1-29 page 20; Table 14-7, page 305).
Tuesday, April 7, 2009
Tuesday April 7, 2009
Q; 32 year old male - recently immigrated from Africa - presented with hypotension and left flank pain and "Milky Urine". What are treatment options beside resuscitation?
Answer: Chyluria (Milky Urine) is common in many parts of the world, where Wuchereria bancrofti, the main agent of filariasis, is endemic. It occurs, on average, 5–10 years after the worm has died, and so there may be no evidence of active filariasis.
Treatment includes therapeutic trial of diethylcarbamazine should be considered before undertaking surgery for lymphatic urinary fistula.
Reference:
1. Filarial chyluria: Long-term experience of a university hospital in India - International Journal of Urology, Volume 11 Issue 4, Pages 193 - 198, Published Online: 16 Mar 2004
Q; 32 year old male - recently immigrated from Africa - presented with hypotension and left flank pain and "Milky Urine". What are treatment options beside resuscitation?
Answer: Chyluria (Milky Urine) is common in many parts of the world, where Wuchereria bancrofti, the main agent of filariasis, is endemic. It occurs, on average, 5–10 years after the worm has died, and so there may be no evidence of active filariasis.
Treatment includes therapeutic trial of diethylcarbamazine should be considered before undertaking surgery for lymphatic urinary fistula.
Reference:
1. Filarial chyluria: Long-term experience of a university hospital in India - International Journal of Urology, Volume 11 Issue 4, Pages 193 - 198, Published Online: 16 Mar 2004
Monday, April 6, 2009
Monday April 6, 2009
Q; What amount of air is usually needed to cause clinical symptoms in Venous Air Emboilsm (VAE)?
Answer: Around 50 ml
But again, all precautions should be taken to avoid even any small amount of air to get introduce into vascular system as there are case reports in literature showing lethal effect with as little as 20 mL of air (the length of an unprimed IV infusion set) or even 0.5 mL of air in the left anterior descending coronary artery causing ventricular fibrillation. Related previous pearl: Venous Air Embolism - VAE - immediate maneuvers Reference: Venous Air Embolism - emedicine.com Most occurrences of VAE go unreported because they are asymptomatic due to very small amount of air entering system, but entrapment of large quantities of intravascular gas may lead to severe neurologic injury, cardiovascular collapse, or even death. The factors that determine the subsequent morbidity and mortality include the rate of air entrainment, the volume of air introduced, and the position of the patient at the time of the embolism. Although very small volumes of air can lead to severe sequelae, generally it is accepted that atleast 50 mL of air is required to cause clinical symptoms.
Sunday, April 5, 2009
Sunday April 5, 2009
Q; You inserted a central venous line in a patient with hypoxemic respiratory failure. Procedure went uneventful. Post-procedure CXR is below. What's your concern?

Answer: Arterial Cannulation
Notice - the catheter is taking a sharp left turn just distal to the clavicle.
The best approach in such situation is to obtain radial ABG and ABG from central line to compare. Also to hook central line to monitor to see waveform which may clearly show arterial waveforms.
Q; You inserted a central venous line in a patient with hypoxemic respiratory failure. Procedure went uneventful. Post-procedure CXR is below. What's your concern?
Answer: Arterial Cannulation
Notice - the catheter is taking a sharp left turn just distal to the clavicle.
The best approach in such situation is to obtain radial ABG and ABG from central line to compare. Also to hook central line to monitor to see waveform which may clearly show arterial waveforms.
Saturday, April 4, 2009
Friday, April 3, 2009
Friday April 3, 2009 (pediatric pearl)
Q: Does sustained meropenem use have effect on the pattern of Gram-negative bacillus colonization in patients admitted to a tertiary care PICU?
Answer: No
In a prospective study, after a 6-mo baseline period, all children with serious infections admitted to the PICU during the subsequent 2 yrs were administered meropenem
.
During the period of preferred meropenem use, the amount of meropenem used increased me than orseven-fold, whereas the use of other advanced generation beta-lactams was reduced by nearly 80%.
Conclusion:
1. There was no statistically detectable effect on the prevalence of colonization by Gram-negative organisms resistant to one or more classes of broad-spectrum parenteral antibiotics
2. or to colonization by organisms resistant specifically to meropenem, when meropenem was the preferred antibiotic in a PICU.
3. The incidence of nosocomial infections did not change, and the prevalence of nosocomial infections caused by meropenem-resistant organisms was always less than 1% of all admissions during the period of meropenem preference.
Reference: click to get abstract
Meropenem use and colonization by antibiotic-resistant Gram-negative bacilli in a pediatric intensive care unit - Pediatric Critical Care Medicine:Volume 10(1)January 2009pp 49-54
Q: Does sustained meropenem use have effect on the pattern of Gram-negative bacillus colonization in patients admitted to a tertiary care PICU?
Answer: No
In a prospective study, after a 6-mo baseline period, all children with serious infections admitted to the PICU during the subsequent 2 yrs were administered meropenem
.
During the period of preferred meropenem use, the amount of meropenem used increased me than orseven-fold, whereas the use of other advanced generation beta-lactams was reduced by nearly 80%.
Conclusion:
1. There was no statistically detectable effect on the prevalence of colonization by Gram-negative organisms resistant to one or more classes of broad-spectrum parenteral antibiotics
2. or to colonization by organisms resistant specifically to meropenem, when meropenem was the preferred antibiotic in a PICU.
3. The incidence of nosocomial infections did not change, and the prevalence of nosocomial infections caused by meropenem-resistant organisms was always less than 1% of all admissions during the period of meropenem preference.
Reference: click to get abstract
Meropenem use and colonization by antibiotic-resistant Gram-negative bacilli in a pediatric intensive care unit - Pediatric Critical Care Medicine:Volume 10(1)January 2009pp 49-54
Thursday, April 2, 2009
Wednesday, April 1, 2009
Wednesday April 1, 2009
LOW DOSE VITAMIN K: DOES IT DECREASES RISK OF BLEEDING
Recent article published in Annals of Internal Medicine by Crowther helps to sort this practice. Low-dose oral vitamin K decreases the international normalized ratio (INR) but its effects on bleeding events are uncertain.
OBJECTIVE: To see whether low-dose oral vitamin K reduces bleeding events over 90 days in patients with warfarin-associated coagulopathy.
DESIGN: Multicenter, randomized, placebo-controlled trial with 14 anticoagulant therapy clinics in Canada, the United States, and Italy.
Method: Nonbleeding patients with INR values of 4.5 to 10.0 either received oral vitamin K, 1.25 mg (355 patients randomly assigned; 347 analyzed), or matching placebo (369 patients randomly assigned; 365 analyzed). Bleeding events (primary outcome), thromboembolism, and death (secondary outcomes) were measured.
Results: 56 patients (15.8%) in the vitamin K group and 60 patients (16.3%) in the placebo group had at least 1 bleeding complication. Major bleeding events occurred in 9 patients (2.5%) in the vitamin K group and 4 patients (1.1%) in the placebo group (absolute difference, 1.5 percentage points [CI, -0.8 to 3.7 percentage points]). Thromboembolism occurred in 4 patients (1.1%) in the vitamin K group and 3 patients (0.8%) in the placebo group (absolute difference, 0.3 percentage point [CI, -1.4 to 2.0 percentage points]). The day after treatment, the INR had decreased by a mean of 1.4 in the placebo group and 2.8 in the vitamin K group.
Limitation: Patients who were actively bleeding were not included, and warfarin dosing after enrollment was not mandated or followed.
CONCLUSION: Low-dose oral vitamin K did not reduce bleeding in warfarin recipients with INRs of 4.5 to 10.0.
Reference: click to get abstract
Crowther MA, Ageno W, Garcia D, Wang L et al. Oral vitamin K versus placebo to correct excessive anticoagulation in patients receiving warfarin: a randomized trial. Ann Intern Med. 2009; 150(5):293-300
LOW DOSE VITAMIN K: DOES IT DECREASES RISK OF BLEEDING
Recent article published in Annals of Internal Medicine by Crowther helps to sort this practice. Low-dose oral vitamin K decreases the international normalized ratio (INR) but its effects on bleeding events are uncertain.
OBJECTIVE: To see whether low-dose oral vitamin K reduces bleeding events over 90 days in patients with warfarin-associated coagulopathy.
DESIGN: Multicenter, randomized, placebo-controlled trial with 14 anticoagulant therapy clinics in Canada, the United States, and Italy.
Method: Nonbleeding patients with INR values of 4.5 to 10.0 either received oral vitamin K, 1.25 mg (355 patients randomly assigned; 347 analyzed), or matching placebo (369 patients randomly assigned; 365 analyzed). Bleeding events (primary outcome), thromboembolism, and death (secondary outcomes) were measured.
Results: 56 patients (15.8%) in the vitamin K group and 60 patients (16.3%) in the placebo group had at least 1 bleeding complication. Major bleeding events occurred in 9 patients (2.5%) in the vitamin K group and 4 patients (1.1%) in the placebo group (absolute difference, 1.5 percentage points [CI, -0.8 to 3.7 percentage points]). Thromboembolism occurred in 4 patients (1.1%) in the vitamin K group and 3 patients (0.8%) in the placebo group (absolute difference, 0.3 percentage point [CI, -1.4 to 2.0 percentage points]). The day after treatment, the INR had decreased by a mean of 1.4 in the placebo group and 2.8 in the vitamin K group.
Limitation: Patients who were actively bleeding were not included, and warfarin dosing after enrollment was not mandated or followed.
CONCLUSION: Low-dose oral vitamin K did not reduce bleeding in warfarin recipients with INRs of 4.5 to 10.0.
Reference: click to get abstract
Crowther MA, Ageno W, Garcia D, Wang L et al. Oral vitamin K versus placebo to correct excessive anticoagulation in patients receiving warfarin: a randomized trial. Ann Intern Med. 2009; 150(5):293-300
Subscribe to:
Comments (Atom)